Introduction
Ligament injuries and fractures of the lower extremities considerably restrict the patients’ freedom of movement and thus their quality of life. Common types of injury are cruciate ligament ruptures and fractures of the upper ankle joint. This particularly affects athletically active people who subsequently want to regain full weight-bearing capacity and functional mobility as quickly as possible.
In this article, we present how mobile gait analysis and biofeedback training based on the Moticon ReGo sensor insoles help to objectively visualize the treatment success in this context. For therapists and patients, gait analysis and biofeedback offer the chance to go through the first phase of rehabilitation as purposefully, quickly and without complications as possible.
Relevance
Until now, gait analyses were tied to laboratories or special premises and to complicated and time-consuming equipment.
In contrast, the Moticon ReGo system offers an efficient and cost-effective alternative for daily use in the practice due to its simple handling and fully automated data analysis. Only the wireless ReGo sensor insoles and the ReGo app are required for use on patients.
The ReGo report parameters from the gait analysis are used to describe the load situation and the load distribution in the real course of movement as well as to display spatial or temporal parameters such as the step length or ground contact times. This enables therapists to identify existing asymmetries and other abnormalities in the patient’s gait pattern and subsequently develop individualized rehabilitation programs or intervene in a targeted manner on the basis of these objective results.
In addition, the use of biofeedback has a positive effect on the success of treatment. It has been used in rehabilitation for about 30 years to support the relearning of movement patterns after injuries, for example that of a stable gait pattern (1). Its use can thus improve the rehabilitation process and reduce the occurrence of complications. A systematic review (1) confirms the effectiveness of biofeedback training in patients with various conditions who exhibit gait abnormalities.
Generally, prescribed partial weight-bearing in trauma patients has been verbally communicated and only selectively practiced with the aid of a body scale. In contrast, the ReGo biofeedback functions offer the opportunity to train and check the partial weight-bearing continuously during the execution of the movement and to involve the patients directly. This can further enhance the quality of treatment outcomes and patient satisfaction. A study by van Lieshout et al (2) confirms that the Moticon ReGo system provides valid feedback data compared to force plates.
A study by Hershhko et al (3) demonstrated that gait rehabilitation with biofeedback was more effective because patients were better able to maintain load limits than those patients who received only verbal instruction. In another study, continuous biofeedback was shown to be more effective than the use of a body scale in maintaining load limits (4).
Study/Case Description
In the present example, a 12-year-old female track and field athlete suffered a slipped right femoral head (epiphysiolysis capitis femoris). As described in the cover article of the Journal for Physical Therapists, the injury was surgically treated by repositioning and screw fixation with a SCEFE screw. Over eight weeks, weight bearing on the affected leg was gradually increased from complete unloading, to sole contact and then partial weight-bearing, each using forearm crutches, to full weight-bearing.
In the period from 23.07.2022 to 11.10.2022, a total of 21 therapy-accompanying Moticon ReGo gait tests were performed for gait analysis. In 15 gait tests, the integrated ReGo biofeedback was also used to actively support the patient’s loading phase and gait training.
In the first phase with unloading and partial loading, the ReGo biofeedback function was first used to control the loads. As biofeedback, two different tones are emitted in real time, respectively when the limit for partial loading is approached and exceeded. The limits were set to 20 kg and 30 kg, respectively, in the ReGo app before performing the gait tests.
In the second phase, from full loading of the injured leg, the ReGo biofeedback function was used to train the physiological rolling of the foot. In the ReGo app, the target end position for rolling in the forefoot can be set for this purpose. During the performance of the gait tests, two different tones were again emitted for approaching and exceeding the limit. The variable limits allowed the patient to be gradually introduced to full roll-off during rehabilitation.
Conservative rehabilitation applied in addition to gait analysis and biofeedback included the following measures:
- Manual lymphatic drainage
- Scar treatment
- Functional mobilization of adjacent joints
- Tension balancing on the muscular, ligamentous and fascial level in the hip-pelvis area
- Extension of hip joint mobility
- Strength training of the muscles surrounding the hip and the trunk
Outcomes
The load histogram shows that the patient adhered to the partial load limit of 20 kg on the right leg. In the Mean Pressure Distribution figure, there is still a noticeable pressure peak in the right forefoot from the time of full load in the test of 15.09.2022, but this normalizes by the time of the last test. Likewise, the force curves (Ground Reaction Force) assume a symmetrical picture from the time of full loading, with two maxima for the heel strike and the impression from the forefoot.
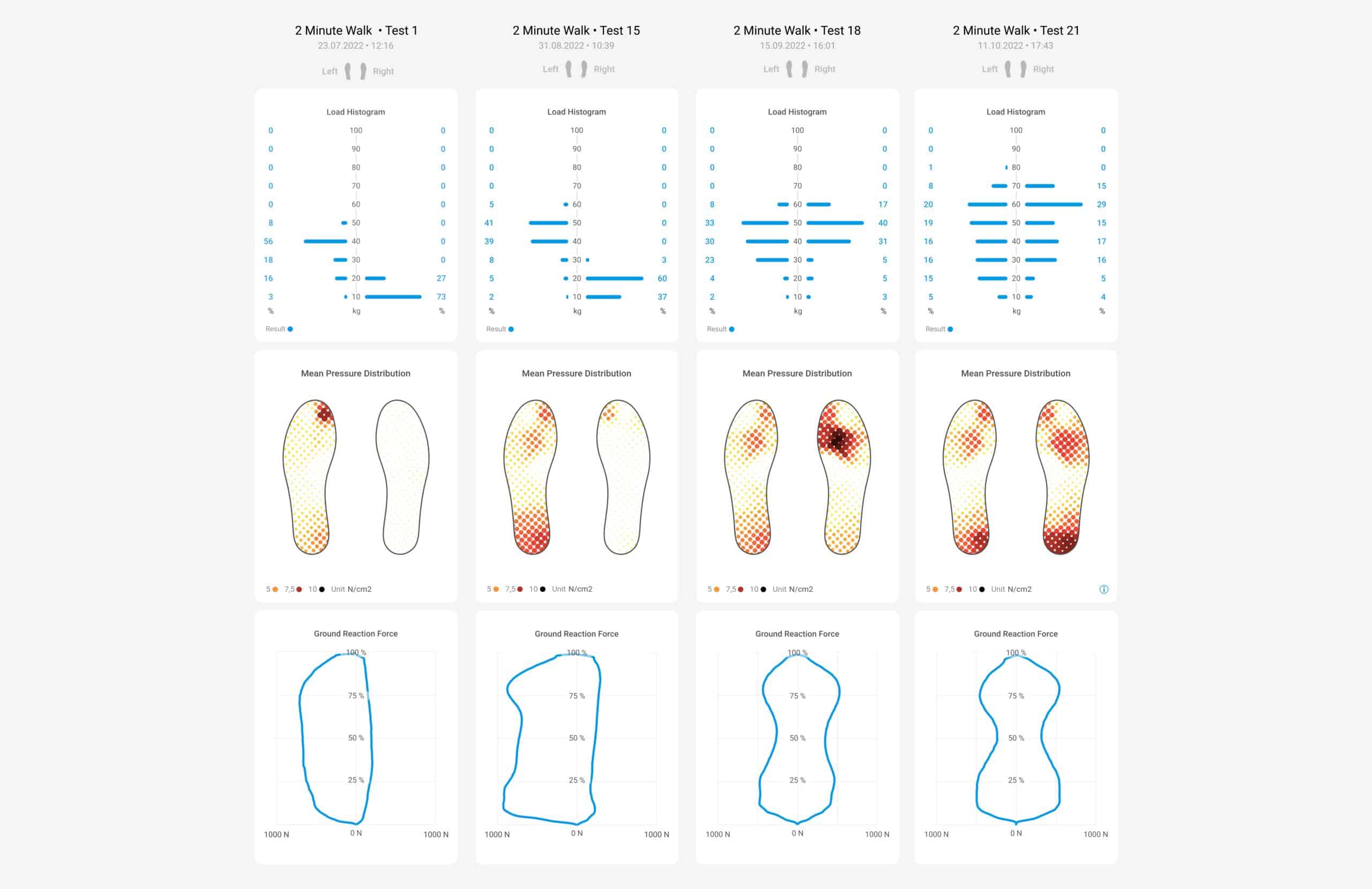
The mean gait line shows the rolling behavior of the foot in the anterior-posterior and transverse directions. In the test of 23.07.2022, a shortened gait line can be seen in the forefoot and rearfoot, indicating that the foot was placed carefully and centrally on the ground due to the partial load. Similarly, the initial/final ground contact points show a significant scatter at the first test, which decreases over time, making the gait pattern more stable and uniform.

All of the above parameters and others (e.g., number of steps, step length) can be plotted over time for the purpose of progress monitoring over several tests. The figure clearly shows the transition from partial loading to full loading of the right leg. Furthermore, the symmetry index (LSI) is shown, which also increases over time.

Discussion
In summary, these data indicate the success of the rehabilitation measures. However, the results of the tests in the course of rehabilitation can also be used in physiotherapy to intervene specifically in the event of abnormalities.
For instance, in the current example, it can be seen in the test of 23.07.2022 that the mean gait line of the right foot is, on the one hand, shortened, as already described above, and also assumes a lateral tendency. This indicates that the patient, presumably due to a protective posture, rolled rather laterally and incompletely over the foot. Subsequently, this was taken into account in the rehabilitation measures in that rolling over the big toe area was trained, which corresponds to the physiological gait pattern. The complete unrolling was in turn specifically improved by means of the Final Stance training. Final Stance Training is another biofeedback option offered by ReGo in addition to partial weight bearing control. Here, the patient receives auditory or haptic feedback when the body’s center of gravity has moved sufficiently far above the sole during the stance phase, meaning that the patient has rolled sufficiently. Further testing over time shows a much more symmetrical and complete gait line compared with the left foot.
Tips for Real Life
From the case study described here, some intervention recommendations can be derived from a physiotherapeutic perspective.
If the gait line is shortened, as in the current example, the complete rolling, from heel strike to leaving the big toe, should be trained. However, since full sole contact is not possible under partial loading, the muscles involved can be strengthened while sitting, for example.
The calf muscles (Musculus Gastrocnemius and Musculus Soleus) are particularly active in the middle of the stance phase until the toes leave the ground (5) and ensure the increase in vertical support and the progression of the body’s center of gravity (6).
| Indication | Exercise | Description |
| Training of calf muscles during partial loading | Seated calf raise | o Sitting, knees bent 90°, weight resting on thighs o Lift heels and lower slowly to the ground o 12 – 15 repetitions, 2 – 3 sets |
Due to the knee flexion in the sitting position, the soleus muscle in particular is trained during this exercise. This causes a braking of the acceleration in the middle and at the end of the stance phase (6). For this reason, it makes sense to train the soleus muscle eccentrically. To do this, the patient slowly lowers the heel to the ground in the above exercise.
Special Product Features
Finally, we would like to summarize the main advantages of the ReGo system and highlight some particularly helpful features of the ReGo system for working with patients.
The ReGo gait tests offer the following advantages for physical therapists in practice:
- Continuous ReGo testing allows therapists to objectively monitor and document success over the entire course of rehabilitation.
- ReGo gait testing can be performed cost- and time-efficiently at any location, even outside the rehabilitation facility and without an internet connection (offline). ReGo allows physiotherapists maximum local flexibility, e.g. for home visits or changing locations.
- ReGo biofeedback features actively engage patients in gait training, increasing motivation and ultimately quality of outcomes. ReGo thus increases customer loyalty to the physiotherapist and customer satisfaction.
- The standardized ReGo tests and automatic movement recognition ensure comparability of results. Thus, the patient’s treatment progress and thus the effectiveness of the corresponding treatment can be objectively documented. In addition, the results help physiotherapists to individualize the treatment.
- The ReGo system is scientifically validated and offers excellent data quality as a basis for medical testing compared to other systems on the market (7).
- In contrast to wired systems, the ReGo sensor insoles do not influence the patient’s movement. The completely wireless and very flat design enables a realistic capture of the gait pattern.
- The ReGo system can also be used for tele-rehabilitation. The ReGo app offers a special user interface for patients and real-time access to the test results for therapists.
Literature
1. Tate JJ, Milner CE. Real-time kinematic, temporospatial, and kinetic biofeedback during gait retraining in patients: a systematic review. Phys Ther 2010; 90(8):1123–34.
2. van Lieshout R, Stukstette MJ, Bie RA de, Vanwanseele B, Pisters MF. Biofeedback in Partial Weight Bearing: Validity of 3 Different Devices. J Orthop Sports Phys Ther 2016; 46(11):993–1001.
3. Hershko E, Tauber C, Carmeli E. Biofeedback versus physiotherapy in patients with partial weight-bearing. Am J Orthop (Belle Mead NJ) 2008; 37(5):E92-6.
4. Hustedt JW, Blizzard DJ, Baumgaertner MR, Leslie MP, Grauer JN. Is it possible to train patients to limit weight bearing on a lower extremity? Orthopedics 2012; 35(1):e31-7.
5. Tao W, Liu T, Zheng R, Feng H. Gait analysis using wearable sensors. Sensors (Basel) 2012; 12(2):2255–83.
6. Francis CA, Lenz AL, Lenhart RL, Thelen DG. The modulation of forward propulsion, vertical support, and center of pressure by the plantarflexors during human walking. Gait Posture 2013; 38(4):993–7.
7. Cramer LA, Wimmer MA, Malloy P, O’Keefe JA, Knowlton CB, Ferrigno C. Validity and Reliability of the Insole3 Instrumented Shoe Insole for Ground Reaction Force Measurement during Walking and Running. Sensors (Basel) 2022; 22(6).